Explore multiorgan involvement of IgG4-RD
Use this educational tool to learn about varied systemic manifestations of IgG4-RD.3
Use this educational tool to learn about varied systemic manifestations of IgG4-RD.3
INDICATIONS
UPLIZNA® (inebilizumab-cdon) is indicated in adult patients for the treatment of: anti-aquaporin-4 (AQP4) antibody positive neuromyelitis optica spectrum disorder (NMOSD); Immunoglobulin G4-related disease (IgG4-RD); anti-...
Use this educational tool to learn about varied systemic manifestations of IgG4-RD.3
Use this educational tool to learn about varied systemic manifestations of IgG4-RD.3
and organ involvement. This informs which specialists, including rheumatologists, gastroenterologists, and ophthalmologists, among others, co-manage patients with IgG4-RD to improve patient outcomes.2
Multiorgan involvement cannot necessarily be ascertained via IgG4-RD symptomatology.4,5 Rather, a combined clinical, imaging, laboratory, and histopathologic assessment should be conducted.2
Get the latest UPLIZNA information and resources as soon as they are available.
Learn about the selective targeting of UPLIZNA as a CD19+ B-cell depleter.
IgG4-RD is a systemic disease with a heterogeneous presentation. Organ involvement and manifestations are highly variable among patients.3,4,6
Take a closer look at IgG4-RD manifestations through the lens of each phenotype and affected organ systems.
Explore the potential manifestations of each phenotype by making a selection from the list below or clicking through the arrows above.
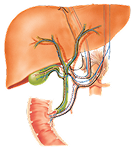
IgG4-related pancreato-hepatobiliary disease may be characterized by pancreatic, liver, and biliary manifestations.7 A greater incidence of diabetes mellitus compared to other phenotypes is likely due to pancreato-biliary involvement.8
Learn more
 Commonly affected organs
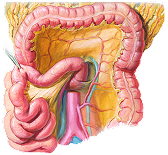
Commonly affected organsIgG4-related retroperitoneal fibrosis and/or aortitis disease often involves manifestations in the retroperitoneum and/or abdominal aorta.7,9 Lymph node involvement can be seen as well.7
Learn more
Commonly affected organsIgG4-RD of the head and neck may be characterized by lacrimal, submandibular, and lymph node involvement.7 This phenotype may be considered more difficult to treat than others and is associated with a higher rate of disease relapse.8
Learn more
Commonly affected organsIgG4-related Mikulicz syndrome with systemic involvement is characterized by combined submandibular, parotid, and lacrimal involvement.7 This phenotype presents with a greater average number of affected organs than other phenotypes.7 Mukulicz/systemic involvement might also include organs more typically associated with other IgG4-RD phenotypes.9
Learn more
Commonly affected organsORGAN SYSTEMS
Pancreatic manifestations of IgG4-RD may include diabetes mellitus and pancreatic enlargement.9,10 Additionally, irreversible pancreatic exocrine insufficiency may cause malabsorption resulting in dramatic weight loss.3,9,10
Patients often experience pancreatic failure before diagnosis of IgG4-RD can be established.3

Manifestations
Related organs
ORGAN SYSTEMS
Hepatobiliary manifestations of IgG4-RD may include diffuse biliary wall thickening, biliary stricture, infectious cholangitis, or hepatic failure.3,9
Manifestations
Related organs
ORGAN SYSTEMS
IgG4-RD manifestation in the aorta can cause thickening of the aortic wall that may result in aneurysms.4,9,10 This can potentially lead to coronary artery disease and constrictive pericarditis.4,9,10 Vessel wall inflammation may cause arterial dissections.4,9,10
Manifestations
Related organs
ORGAN SYSTEMS
Retroperitoneal manifestations of IgG4-RD may include renal atrophy or injury due to hydronephrosis.9
Retroperitoneal fibrosis associated with IgG4-RD may potentially lead to irreversible nerve damage, abdominal and back pain, difficulty urinating, or renal failure.10,11
The retroperitoneum is among the most frequent sites involved in IgG4-RD.3
Manifestations
Related organs
ORGAN SYSTEMS
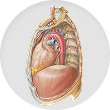
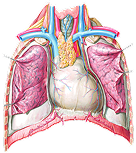
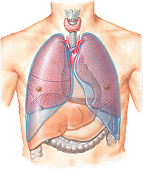
IgG4-RD may cause fibrosing mediastinitis that results in compression of local structures within the mediastinum, including the esophagus, heart, and thoracic aorta, and shortness of breath.4,9
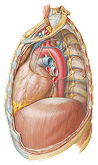
Manifestations
Related organs
ORGAN SYSTEMS
IgG4-RD manifestations in the skull, sinuses, and ears may include midline destructive lesions, anosmia, bone destruction, chronic sinusitis, and hearing loss.9 Sinonasal masses are also possible.12

Manifestations
Related organs
ORGAN SYSTEMS
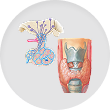
IgG4-RD often presents with organ enlargement resembling tumors.3 Presentation in the thyroid or pituitary gland can result in hypothyroidism or hypopituitarism, respectively.9

Manifestations
Related organs
ORGAN SYSTEMS
IgG4-RD associated masses and muscle myositis in the eye sockets and orbital area may result in proptosis, diplopia, and eyelid swelling, potentially leading to vision loss.4,5,9
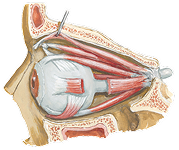
Manifestations
Related organs
ORGAN SYSTEMS
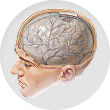
Inflammation caused by IgG4-RD may lead to thickening of the pachymeninges, which can cause cranial nerve palsies, neurologic deficits, and seizures.4,9,10
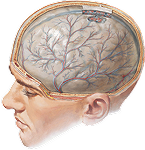
Manifestations
Related organs
ORGAN SYSTEMS
The salivary and lacrimal glands are among the most frequent sites involved in IgG4-RD.3 Manifestations may include sicca or symmetric enlargement of the lacrimal and some major salivary glands (Mikulicz syndrome).3,9,11
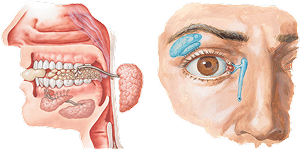
Manifestations
Related organs
ORGAN SYSTEMS
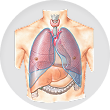
IgG4-RD may lead to pulmonary fibrosis, interstitial lung disease, diffuse thickening of the bronchus, or pleural effusion.3,5,9 Potential masses, nodules, bronchial wall thickening, and inflammation and fibrosis of the lung tissue may result in cough and fatigue.3,5,9
Manifestations
Related organs
ORGAN SYSTEMS
Renal manifestations of IgG4-RD may include tubulointerstitial nephritis, renal failure due to interstitial or glomerulonephritis, potentially irreversible chronic kidney disease, and blood in the urine.4,9,10 Additionally, focal masses, usually multiple, may cause enlargement and blockage of urinary flow.3,4,9,10

Manifestations
Related organs
Discover how UPLIZNA may help.
Primary Endpoint

7 out of 68 patients on UPLIZNA (10.3%) experienced IgG4-RD flares vs 40 out of 67 patients on placebo (59.7%) at Week 52 (HR: 0.13 [95% CI: 0.06, 0.28]; P<0.0001)13

40 out of 68 patients on UPLIZNA (58.8%) achieved steroid-free, flare-free complete remission vs 15 out of 67 patients on placebo (22.4%) at Week 52 (difference: 36.5% [95% CI: 21.0%, 51.9%]; P<0.0001)13,‡
*Complete remission was defined as an IgG4-RD Responder Index score of 0 or attestation by the
investigator that there was no clinical evidence of active disease.
†Excluding the required 8-week steroid taper in all patients.
‡Based on logistic regression model, with placebo as the reference group.
The most common adverse reactions with UPLIZNA were urinary tract infection and lymphopenia13
After 2 initial doses on Day 1 and Day 15, UPLIZNA is administered as 1 dose every 6 months. Each infusion is administered over ~90 minutes.13
Phenotypes:
IgG4-related pancreato-hepatobiliary disease may be characterized by pancreatic, liver, and biliary manifestations.7 A greater incidence of diabetes mellitus compared to other phenotypes is likely due to pancreato-biliary involvement.8
Commonly affected organs and select possible manifestations
Organ involvement and clinical manifestations of IgG4-RD vary among patients. The organs listed above may not be affected in all patients.3,4,6
Phenotypes:
IgG4-related retroperitoneal fibrosis and/or aortitis disease often involves manifestations in the retroperitoneum and/or abdominal aorta.7,9 Lymph node involvement can be seen as well.7
Commonly affected organs and select possible manifestations
Phenotypes:
IgG4-RD of the head and neck may be characterized by lacrimal, submandibular, and lymph node involvement.7 This phenotype may be considered more difficult to treat than others and is associated with a higher rate of disease relapse.8
Commonly affected organs and select possible manifestations
Phenotypes:
IgG4-related Mikulicz syndrome with systemic involvement is characterized by combined submandibular, parotid, and lacrimal involvement.7 This phenotype presents with a greater average number of affected organs than other phenotypes.7 Mukulicz/systemic involvement might also include organs more typically associated with other IgG4-RD phenotypes.9
Commonly affected organs and select possible manifestations
IgG4-RD, immunoglobulin G4–related disease; MOA, mechanism of action.
IMPORTANT SAFETY INFORMATION AND INDICATIONS
CONTRAINDICATIONS
UPLIZNA® (inebilizumab-cdon) is contraindicated in patients with a history of a life-threatening infusion reaction to UPLIZNA, active hepatitis B infection, or active or untreated latent tuberculosis.
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
INDICATIONS
UPLIZNA® (inebilizumab-cdon) is indicated in adult patients for the treatment of: anti-aquaporin-4 (AQP4) antibody positive neuromyelitis optica spectrum disorder (NMOSD); Immunoglobulin G4-related disease (IgG4-RD); anti-acetylcholine receptor (AChR) or anti-muscle specific tyrosine kinase (MuSK) antibody positive (Ab+) generalized myasthenia gravis (gMG).
Please see UPLIZNA Full Prescribing Information.
IMPORTANT SAFETY INFORMATION AND INDICATIONS
CONTRAINDICATIONS
UPLIZNA® (inebilizumab-cdon) is contraindicated in patients with a history of a life-threatening infusion reaction to UPLIZNA, active hepatitis B infection, or active or untreated latent tuberculosis.
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
INDICATIONS
UPLIZNA® (inebilizumab-cdon) is indicated in adult patients for the treatment of: anti-aquaporin-4 (AQP4) antibody positive neuromyelitis optica spectrum disorder (NMOSD); Immunoglobulin G4-related disease (IgG4-RD); anti-acetylcholine receptor (AChR) or anti-muscle specific tyrosine kinase (MuSK) antibody positive (Ab+) generalized myasthenia gravis (gMG).
Please see UPLIZNA Full Prescribing Information.